Overall, the manifestation of Marco's disease improved greatly and his neuromuscular functioning made gains. Consequently, his American Spinal Injury Association (ASIA) score further improved from grade C at the beginning of the Rehab-Cycle® to grade D at the final assessment. This meant that in addition to having motor functioning below the affected level of the spinal cord and more than half of key muscles the ability to undergo active movement with full range of motion, these muscle activities were also able to be executed with gravity and with moderate resistance in specific positions. The paraplegia experienced by Marco evolved from complete paraplegia at admission to incomplete paraplegia at the final assessment/evaluation.
""The paraplegia experienced by Marco evolved from complete paraplegia at admission to incomplete paraplegia at the final assessment/evaluation.""
To evaluate the changes in Marco's functioning a final assessment of the intervention targets was performed. The results of the final assessment is illustrated on the ICF Evaluation Display, a visual depiction of the results from the first and the final assessment as well as goal achievement. As with Marco's ICF Categorical Profile BITTE HIER EINEN ANKER ZUM CATEGORICAL PROFILE UNTER SECTION GOAL-SETTING/DETERMINATION..., the ICF Evaluation Display employs bar charts to depict Marco's functioning at two time points – at the first assessment and at the final assessment. The ICF Evaluation Display also shows whether the goals set during the assessment phase were achieved after intervention. It is important to note that the comparison of the first and final ratings only imply that there was a change, not whether the change was due to the interventions conducted. Likewise, goal achievement did not imply that reaching or not reaching the goal was due to interventions. See table 4.
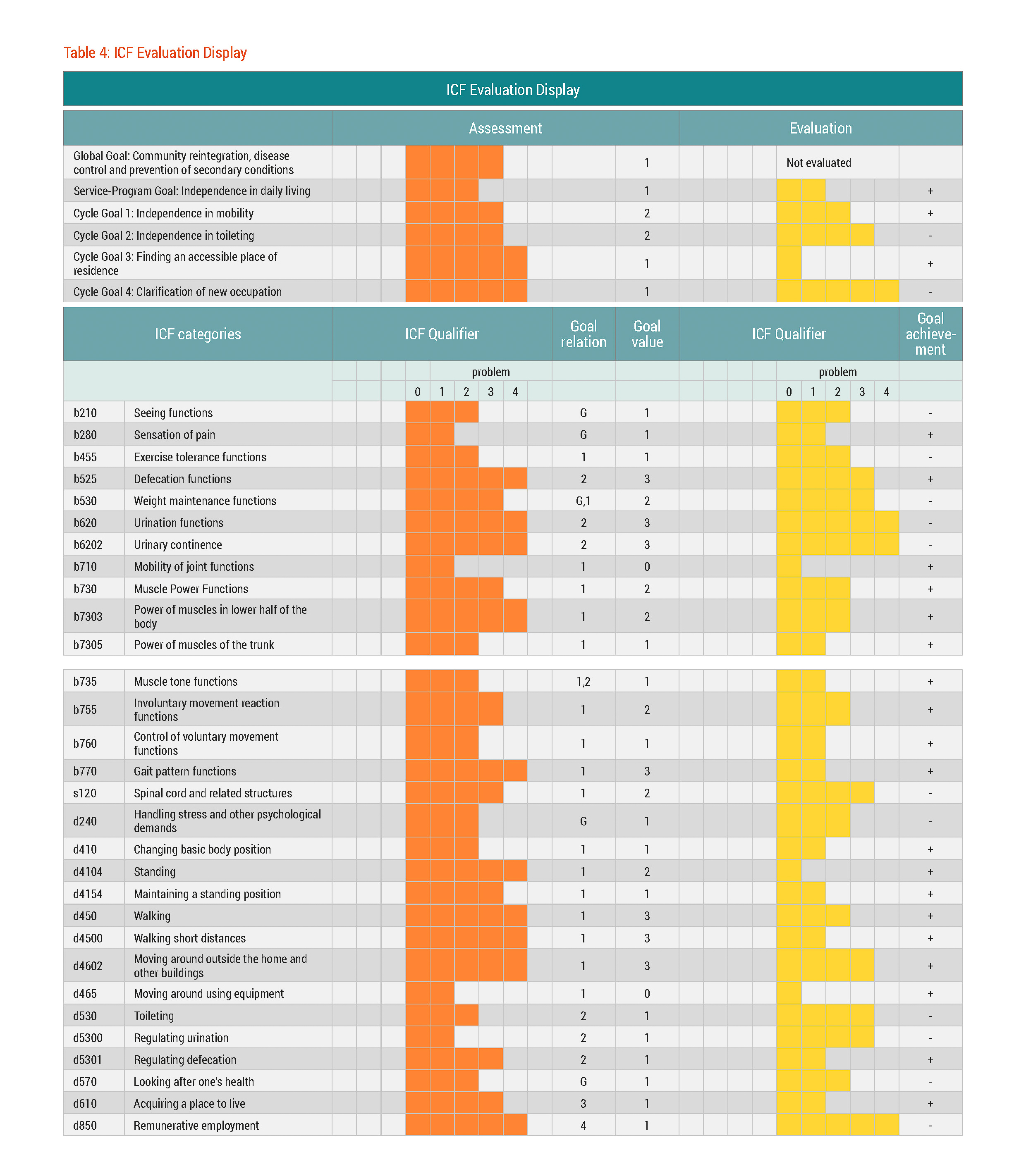
Marco achieved success in reaching cycle goal 1 ‘independence in mobility’ and cycle goal 3 ‘finding an accessible place of residence’.
With the assistance of the occupational therapist and some of his friends, Marco secured a new apartment that was also wheelchair accessible. Having a place to live alleviated some of the stress that Marco had been dealing with since the onset of his disease.
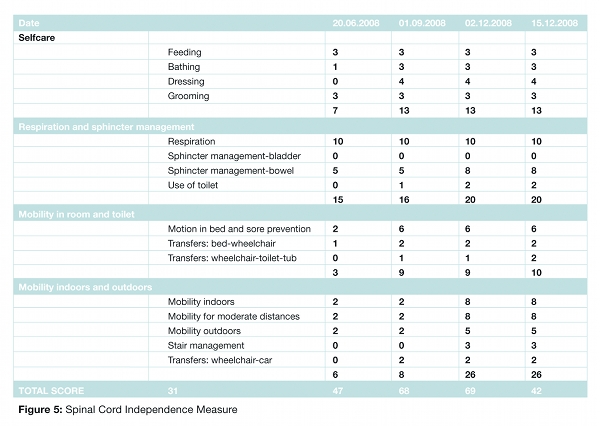
At the final assessment, Marco was able to walk short distances with increasing dexterity. Despite continued need to increase muscle power, his muscle power improved in both the lower extremities and the trunk. Further increase in muscle power was expected to alleviate the residual impairments in gait pattern functions. His muscle tone functions improved as well, with fewer involuntary movements and greater control over voluntary movement. Improved mobility enabled Marco to more independently use the toilet. These improvements were confirmed by Marco’s steadily rising Spinal Cord Independence Measure (SCIM) score.{cs14-fn15} Marked by improvements in mobility, bowel sphincter management and use of toilet, his SCIM score increased from 46 to 69 throughout the course of the Rehab-Cycle®. See table 5.
While Marco’s bowel functioning had made significant gains, with increased bowel and anal sensitivity and the ability to defecate independently at regular intervals, limited control over defecation in certain situations sometimes led to bowel incontinence.
Now I can feel in my stomach when I need to go. Then I have about ten minutes to find a bathroom because of incontinence. If I’m out, I really need to rush to find a public toilet. I hope this will improve, but perhaps it will stay this way for the rest of my life.
Marco
Unfortunately, Marco’s urinary functioning did not improve at all; the bladder incontinence remained. This was a great disappointment for him. Marco's ability to regulate urination had been hindered by the condom catheter that periodically detached with certain body movements.
The condom catheter was extremely frustrating. It came off all the time – at night, when I was moving around. I tried for months and it just didn’t work. Catheterisation is something I really didn’t want to do – it’s just too uncomfortable, too painful…and I had to do it several times a day. So I have chosen the stent in spite of the risks. It really seemed like the best option for me.
Marco’s thoughts on treatment options for bladder dysfunction
It can take up to six months or so until a person’s body accepts a stent. There’s always a chance that it will be rejected or there will be continuous infections and it will need to be removed, then there are few options left, such as surgically enlarging the bladder and catheterisation. Marco must really be careful about recurring infections.
Marco’s doctor post-surgery
With regard to Marco's seeing functions, he continued to experience reduced sight in his left eye due to the inflammation caused by his disease. Despite overall improvement in the manifestations of the disease, inflammation had returned regularly. To tackle inflammation, doctors recommended a stronger anti-inflammatory therapy i.e. anti-TNF-alpha therapy. This therapy was associated with side effects that also required close monitoring. The combination of the anti-inflammatory drug along with the surgically implanted stent put Marco at increased risk for infection. He did develop a chronic urinary tract infection, but unclear when. Thus, it was essential that Marco and the health professionals who continued to be involved in his healthcare carefully monitored possible signs of disease relapse. This meant that Marco had to take on the responsibility for self-care and eye checks seriously. This was especially important after discharge from the rehabilitation centre to the community.
Although not all of the rehabilitation goals set were achieved, Marco was discharged from the rehabilitation centre to his new apartment. To address his remaining needs, including the exploration of a new occupation – one of the rehabilitation goals not reached during the Rehab-Cycle® – an outpatient rehabilitation programme was organised.