
Assignment
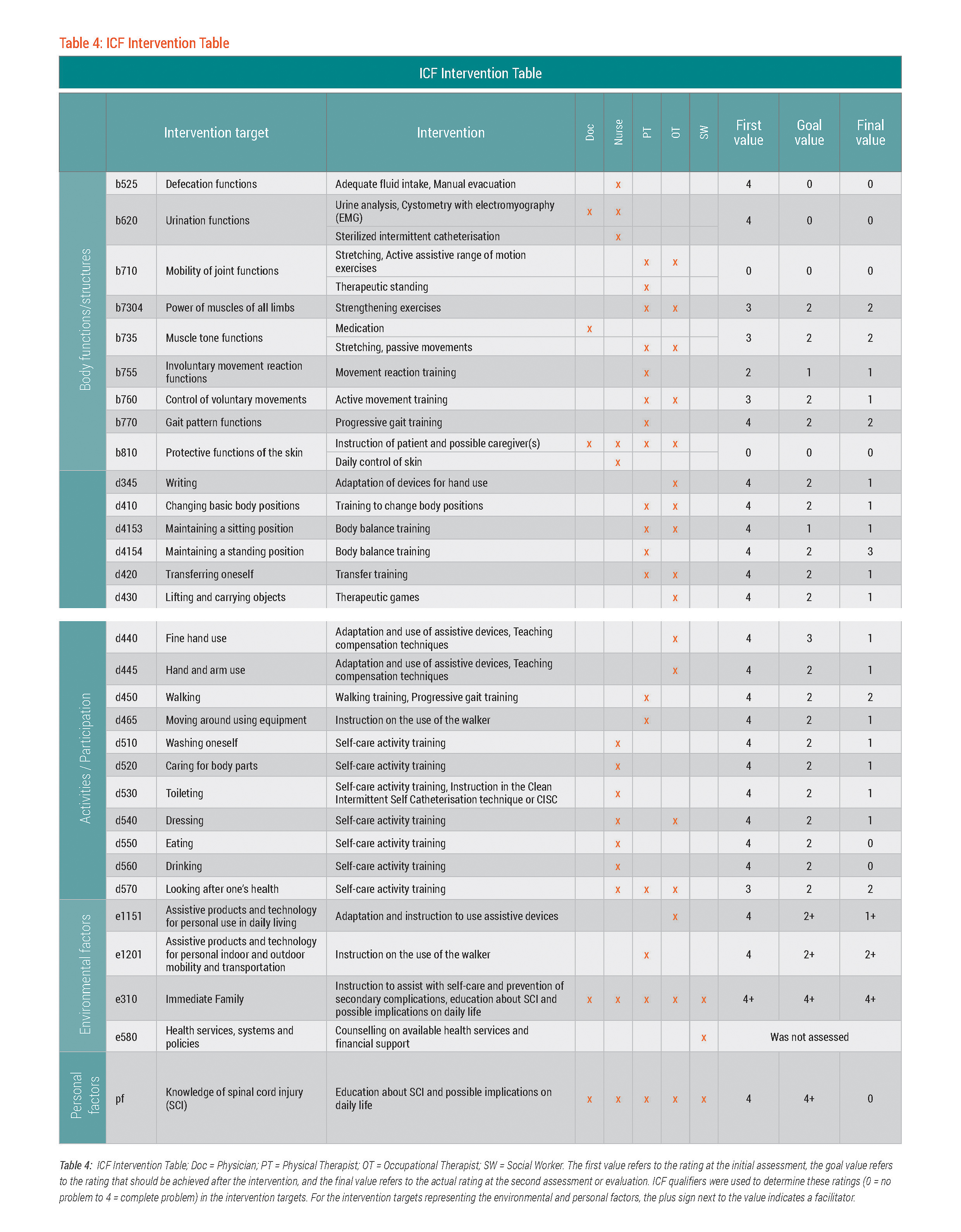
The assignment of the intervention targets to the members of Mr. Dee's rehabilitation team – physician, nurse, physical (PT) and occupational (OT) therapists, and social worker – was documented on the ICF Intervention Table. This table provides an overview of all the intervention targets, the interventions themselves, and the responsible rehabilitation team members. See table 4. The ICF Intervention Table can be used by the team in planning and implementing the appropriate interventions for each intervention target. Having such an overview can help avoid gaps and redundancy in service provision.
Interventions
Some of Mr. Dee's intervention targets were assigned to more than one rehabilitation team member. For example, b735 Muscle tone functions was assigned not only to the physician but also to both the PT and the OT. This made sense since this intervention target related to spasticity is ideally addressed from different perspectives. While the physician focused on the medical aspects of spasticity by prescribing medication and monitoring its effect, the PT and OT dealt predominately with the physiological and movement aspects of spasticity. In Mr. Dee's case, both the PT and OT provided interventions with stretching and passive movement. However, the PT attended to the lower body, while the OT to the upper body.
""While the physician focused on the medical aspects of spasticity by prescribing medication and monitoring its effect, the PT and OT dealt predominately with the physiological and movement aspects of spasticity""
The interventions for improving independence in self-care and for prevention of secondary complications were primarily undertaken by Mr. Dee’s physician and nurse. Regular urine analyses and occasional sterile catheterisation (to empty the bladder) were conducted to compensate for the lack of control over b620 Urination functions. As previously mentioned, medication was also administered to influence the increased muscle tone in the lower extremity. Through one-on-one training, the nurse helped Mr. Dee with improving his execution of self-care activities, such as d510 Washing oneself, d520 Caring for body parts, d540 Dressing, as well as instructed him on strategies for looking after his health (d570) including preventing complications. Moreover, the nurse involved Mr. Dee’s wife during some of the self-care training sessions in order to strengthen the skills she needed to care for Mr. Dee at home.
In addition to the interventions provided by the nurse to prevent complications, all the members of the rehabilitation team took steps to educate Mr. Dee and his wife about spinal cord injury (SCI). Expanding Mr. Dee and his wife's knowledge about SCI was also intended to increase their awareness about possible implications of SCI on their lives.
Mr. Dee’s PT and OT incorporated interventions primarily aimed at improving mobility. Some interventions were provided by both the PT and OT. For example, stretching, passive and active range of motion (ROM) exercises, and strengthening exercises were implemented to improve b710 Mobility of joint functions, b7304 Power of muscles of all limbs, and b735 Muscle tone functions. Some interventions related to mobility were provided solely by the PT e.g. progressive gait training to improve b770 Gait pattern functions or walking with an assistive walker (d465 Moving around using equipment). The interventions provided solely by the OT focused on increasing independence in d430 Lifting and carrying objects, d440 Fine hand use and d445 Hand and arm use e.g. adaptation and use of assistive devices. Related to the mobility of the hands and fingers, the OT also incorporated the adaptation of assistive devices to improve Mr. Dee's writing skills (d345 Writing).
A social worker complemented the rehabilitation team by counselling Mr. Dee on available health services and the healthcare policies that were relevant to his rehabilitation and subsequent community reintegration. The intervention provided by the social worker was only indicated on Mr. Dee's ICF Intervention Table, but not assessed nor indicated on the ICF Categorical Profile((Bitte Anker auf ICF Categorical Profile von Mr. Dee unter Section "Goal-setting/Determination of Intervention Targets")) or the ICF Evaluation Display((Bitte Anker auf ICF Evaluation Display von Mr. Dee unter Section "Evaluation")).
All of these interventions were performed in a rehabilitation setting with limited financial resources. For instance, expensive rehabilitation equipment such as a locomat, a therapeutic swimming pool, and gymnasium were not available. However, the professional and well-trained staff were knowledgeable and resourceful in applying available rehabilitation approaches and techniques that compensated for the inadequacies in infrastructure and equipment. For example, the PT used a hand crank to improve muscle power and a stationary bed for practicing how to optimally change basic body positions, and the OT employed simple, fairly inexpensive devices to train fine hand function, and hand and arm use.
""...the professional and well-trained staff were knowledgeable and resourceful in applying available rehabilitation approaches and techniques that compensated for the inadequacies in infrastructure and equipment.""
The status of Mr. Dee's functioning, as represented by the intervention targets, were evaluated again at the end of the six-week Rehab-Cycle®. The results of the second evaluation are denoted by the final value on the ICF Intervention Table. This final value was also documented as a bar-chart on the ICF Evaluation Display.