
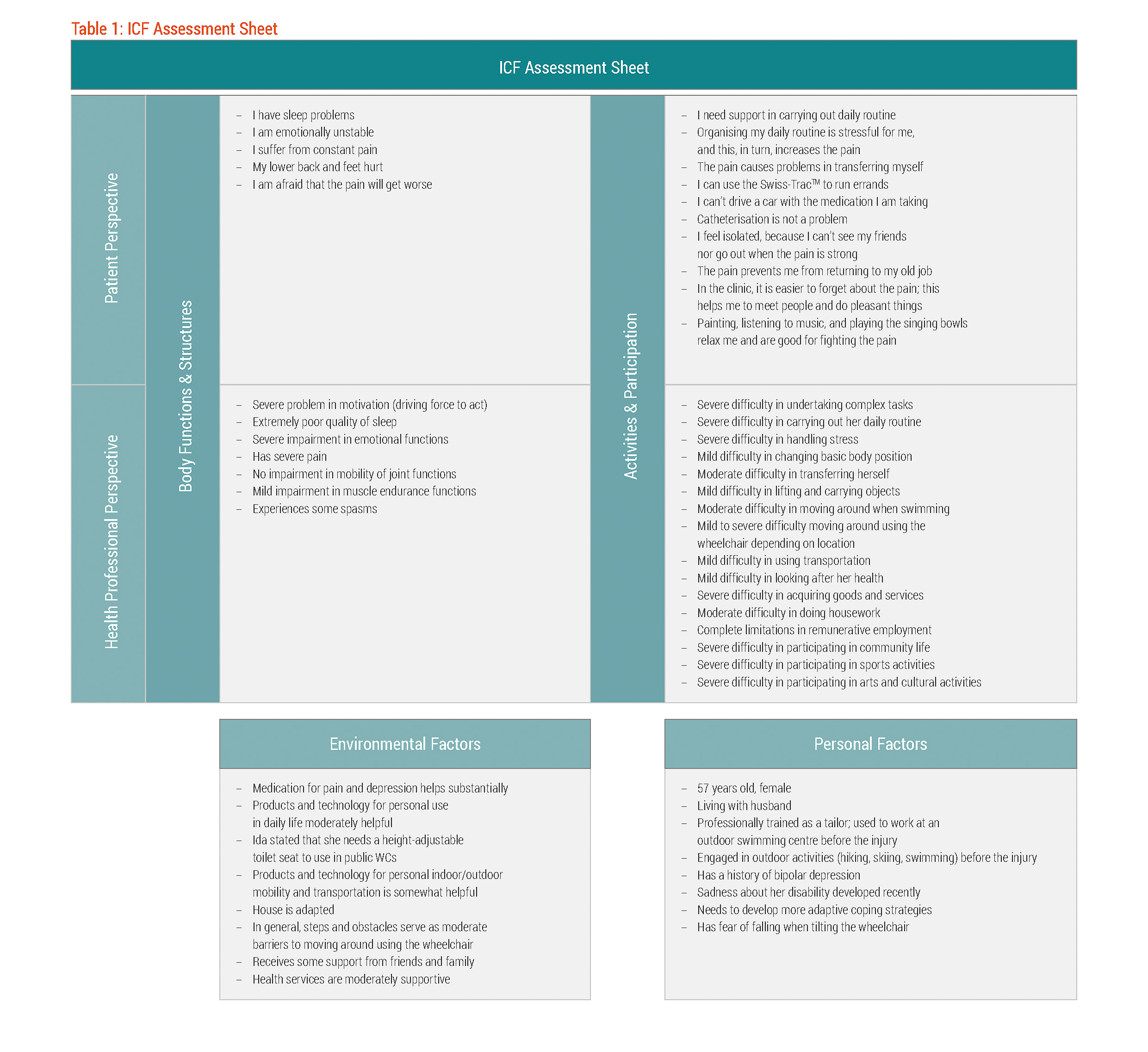
The results of the comprehensive assessment, including selected statements made by Ida about her pain experience and other aspects of functioning, were documented using the ICF Assessment Sheet and according to the World Health Organization's International Classification of Functioning, Disability and Health (ICF).{cs19-fn21} Not only is the ICF a recognised international standard for describing functioning, the utility of using the ICF to capture the biopsychosocial aspects of post-SCI pain is supported in scientific literature.1314 The ICF Assessment Sheet provides a quick overview of the assessment results structured according to the ICF components of body functions and structures, activities and participation, environmental factors, and personal factors. The items place under body functions and structures, and activities and participation were further differentiated by Ida's perspective and the health professional perspective. See table 1.
Body Functions and Structures
Since the impetus for Ida’s rehabilitation was pain management, sensation of pain was logically the focus of the items documented under the ICF component of body functions and structures. Ida has been experiencing constant and severe pain, specifically in her lower back and extending down to her feet. To assess the intensity of pain, the rehabilitation team applied the Visual Analog Scale (VAS).{cs19-fn22}
Box 2 | Measuring Post-SCI Pain
Reliable and valid measures are essential for determining the impact of interventions in the management of post-SCI pain. Post-SCI pain can be assessed according to various domains:{cs19-fn22}{cs19-fn23}
- Pain intensity: how much a person hurts, e.g. extremely painful
- Pain affect: the emotional reaction(s) associated with the pain experience, e.g. fear of worsening pain
- Pain quality: description of how the pain is felt, e.g. burning pain
- Pain location: perceived location of the pain sensation on or in the body, e.g. pain at the lesion area
- Pain interference: extent pain interferes with daily functioning, e.g. cannot sleep due to pain
- Temporal characteristics of pain: variability, frequency, and duration of the pain experience, e.g. constant and unchanging pain
Although all of these domains are important to consider in when assessing pain, pain intensity is considered the primary domain to assess. The most commonly employed measures to assess pain intensity are the Visual Analogue Scale, Numeric Rating Scale, and the Verbal Rating Scale.{cs19-fn22}{cs19-fn23}{cs19-fn24}
- Visual Analogue Scale (VAS): This measure consists of a line, usually 10 cm (or 100 mm) long, that is labelled with “no pain” on one end and the other extreme, e.g. “pain as bad as it could be”, on the other end. The person is asked to indicated any point on the line that best corresponds to the intensity of pain he or she is experiencing. The distance in cm or mm from the “no pain” mark to the point on the line indicated by the person represents the pain intensity.
- Numeric Rating Scale (NRS): The NRS is similar to the VAS. However, the line is numbered along a continuum from 0 to 10 (or 0-100), with “0” corresponding to “no pain” on one end and “10” (or “100”) corresponding to label on the other end. The person is asked to circle or verbally indicate which number best corresponds to the intensity of pain he or she is experiencing. The person is not allowed to indicate a point on the line between the numbers.
- Verbal Rating Scale (VRS): The person is asked to select from a list of adjectives the word or phrase that best describes the intensity of pain he or she is experiencing. The adjectives on the list are generally assigned a score that corresponds with a rank based on pain severity.
Of these three scales, the NRS is the most widely used measure in assessing pain experienced by persons with SCI. It also seems to be the preferred measure of choice – it is easy to understand and use, demonstrates strong scientific validity, and is sensitive to the impact of treatment on the pain experience. Moreover, the 0-10 NRS has been recommended by the IMMPACT initiative as a core outcome measure for clinical trials of chronic pain.{cs19-fn22}{cs19-fn23}{cs19-fn24}
The other domains of pain can be assessed using various measures, e.g. Short-Form McGill Pain Questionnaire to assess pain affect and Leeds Assessment of Neuropathic Signs and Symptoms to assess pain quality.{cs19-fn22}{cs19-fn23}{cs19-fn24} However, detailing these measures would go beyond the scope of this case study.
The rehabilitation team employed a VAS scale that, like the NRS, contained numbers along the continuum from 0 to 10. On this specific VAS scale, Ida rated the intensity of her pain as 8. The rehabilitation team classified the pain as neuropathic.
In terms of pain interference, Ida experienced poor sleep quality, i.e. she would sometimes wake up, due to pain. In terms of pain affect, Ida presented with low motivation, emotional instability, and was afraid that the pain would get worse.
The results of the clinical assessment conducted by the rehabilitation team were consistent with the statements made by Ida about her pain and her functioning. The consistency between Ida's statements about feeling depressed and the psychological evaluation results led to a diagnosis of minor clinical depression, possibly related to a pre-existing bipolar disorder.
Activities and Participation
Regarding the ICF component of activities and participation, Ida experienced major limitations in carrying out her daily routine. This, in turn, stressed Ida out, resulting in an exacerbation of her pain. The rehabilitation team also found that Ida had severe difficulty in undertaking complex tasks and in handling stress.
""Furthermore, although Ida was capable of driving a car, the constant pain and the pain medication she was taking prevented her from driving.""
In terms of mobility, Ida reported that the use of a Swiss-TracTM increased her mobility, enabling her to run errands. Nevertheless, the rehabilitation team saw the potential for problems in running errands due to Ida's difficulties in handling stressful situations. Other mobility-related issues included problems in transferring and driving. Ida reported that transferring to and from the wheelchair was painful; this was supported by the rehabilitation team's assessment. Furthermore, although Ida was capable of driving a car, the constant pain and the pain medication she was taking prevented her from driving.
These mobility problems severely limited her ability to meet friends and hindered her from working. As a result Ida felt isolated.
With regard to self-care, the rehabilitation team found that Ida was independent in completing self-care activities.
Environmental and Personal Factors
There were several environmental factors that served as supports for her. This included the pain medication and antidepressants, a house that was well-adapted to her needs, and a supportive husband. However, there were also environmental factors that served as barriers. For example, the pain medication she was taking had many side effects, and these side effects negatively impacted on her ability to drive a car.
""Ida had problems coping with her pain and overall situation. Moreover, she developed a fear of falling...""
In terms of personal factors, Ida had problems coping with her pain and overall situation. Moreover, she developed a fear of falling following her accident.
Addressing this fear of falling and developing more adaptive coping strategies were among the many intervention targets defined by Ida and the rehabilitation team for this Rehab-Cycle®, and for which specific goals were set.