Structure of the ICF
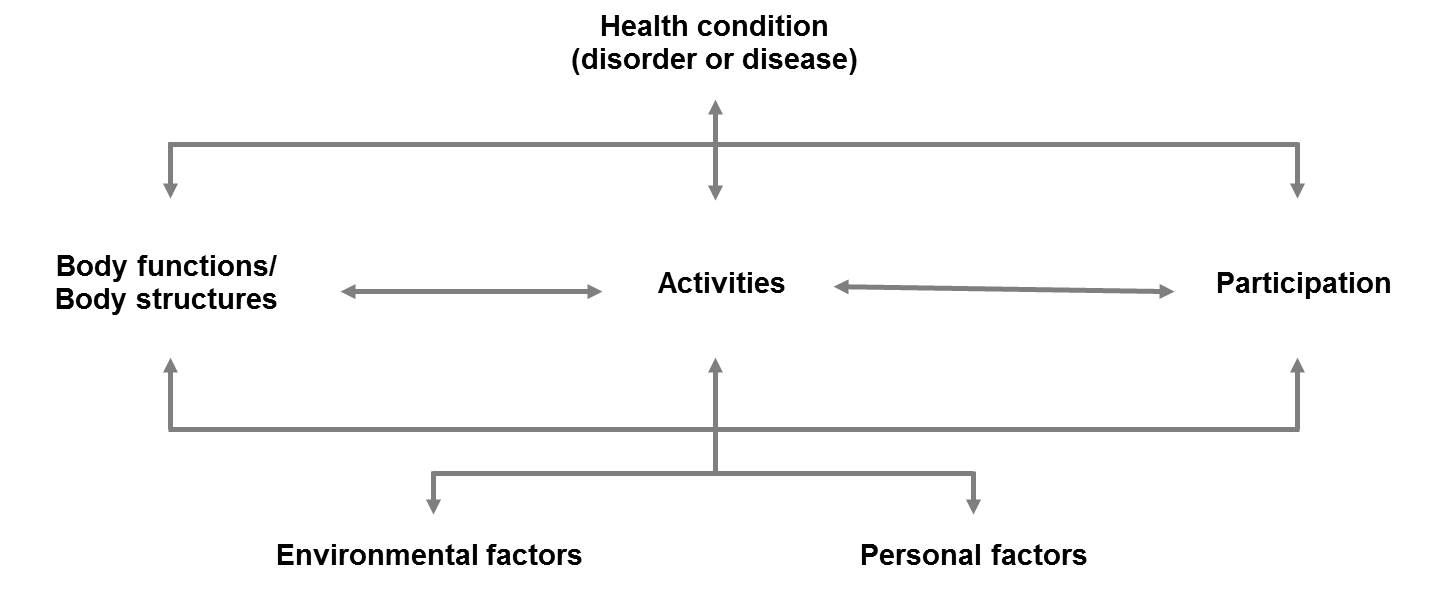
This bio-psycho-social perspective guided the development of the International Classification of Functioning Disability and Health (ICF). As such, the components of the classification correspond to the components of the model. Within each component, there is an exhaustive list of ICF categories that serve as the units of the classification. ICF categories are denoted by unique alphanumeric codes and are hierarchically organized in chapter, second, third and fourth levels. When going from the chapter level to the fourth level, the category's definition becomes more detailed.
ICF categories are arranged in a stem-branch-leaf structure within each component, in which the more detailed level categories share the same attributes as the more broader level categories. Every component consists of chapters, with chapters representing the broadest level. Each chapter then consists of second-level categories, which in turn, are composed of categories at the third level. Some third level categories also include fourth-level categories. This structure can be compared to that of school books, in which the information is usually organized in chapters and subheadings to help locate the information sought.
An example from the component body functions is presented below:
| Code | Level |
|---|
| b2 |
Sensory functions and pain (chapter level) |
| b280 |
Sensation of pain (second level) |
| b2801 |
Pain in body part (third level) |
| b28013 |
Pain in back (fourth level) |
Although the ICF reflects the bio-psycho-social model, there are some differences between the model and the classification. For example, the bio-psycho-social model depicts activities and participation as distinct entities. However, clearly distinguishing between them based on ICF categories is not yet possible given international variation, differing approaches of professionals and theoretical frameworks. For this reason, the ICF keeps activities and participation as one component of functioning. Moreover, although personal factors are included as a component of the bio-psycho-social model, they are not yet classified in the ICF.
ICF Qualifiers
The classification also comprises so-called ICF qualifiers, which quantify the extent of a problem experienced by a person in a specific ICF category. The World Health Organization proposes that the categories in the components of body functions and structures, and activities and participation be quantified using the same generic scale:
| Value | Description |
|---|
| 0 |
NO problem (none, absent, negligible,...) 0-4% |
| 1 |
MILD problem (slight, low,...) 5-24% |
| 2 |
MODERATE problem (medium, fair,...) 25-49% |
| 3 |
SEVERE problem (high, extreme,...) 50-95% |
| 4 |
COMPLETE problem (total,...) 96-100% |
| 8 |
not specified (used when there is insufficient information to quantify the extent of the problem) |
| 9 |
not applicable (used to indicate when a category does not apply to a particular person) |
The ICF qualifier is added to the category following a 'dot' e.g. b280.1 (mild sensation of pain) or b28013.3 (severe pain in the back).
Environmental factors are quantified with a negative and positive scale that denotes the extent to which an environmental factor acts as a barrier or a facilitator:
| Qualifier - Barrier | Qualifer - Facilitator |
|---|
| 0 - NO barrier |
+0 - NO facilitator |
| 1 - MILD barrier |
+1 - MILD facilitator |
| 2 - MODERATE barrier |
+2 - MODERATE facilitator |
| 3 - SEVERE barrier |
+3 - SUBSTANTIAL facilitator |
| 4 - COMPLETE barrier |
+4 - COMPLETE facilitator |
| 8 - barrier, not specified (the environmental factor is a barrier; however there is insufficient information to quantify the extent of the problem) |
+8 - facilitator, not specified (the environmental factor is a facilitator; however there is insufficient information to quantify the extent of the facilitative inpact) |
| 9 - not applicable (used to indicate when a category does not apply to a particular person) |
|
To indicate that an environmental factor serves as a barrier, the ICF qualifier is added to the category following a 'dot' e.g. e150.2 (moderate barrier posed by the design, construction, products and technology of buildings for public use). To indicate that an environmental factor serves as a facilitator, the ICF qualifier is added to the category following a plus sign e.g. e1151+4 (Assistive products and technology for personal use in daily living serves as a complete facilitator).
An ICF qualifier of '8', not specified, is used when it is known that the environmental factor is a barrier, however there is insufficient information to quantify the extent of the problem. Likewise an ICF qualifier of '+8', also not specified, is used when it is known that the environmental factor is a facilitator, however there is insufficient information to quantify the extent of the problem. The ICF qualifier of '9', not applicable, is used in the same way as with the generic scale.
It is important to note that in addition to this generic scale, the ICF contains additional qualifiers specific to the different components. For example, the second and third qualifiers of the component body structures are used to indicate the nature of a body structure change and its location respectively.
The ICF contains more than 1400 categories, making it a highly comprehensive classification. This comprehensiveness is a major advantage and strength of the ICF. It is, however, also the biggest challenge to its practicability. To enhance the applicability of the classification, ICF-based tools must to be tailored to the needs of the users - without weakening the strengths of the ICF. One approach is the development of ICF Core Sets.
Literature
- World Health Organization. International Classification of Functioning, Disability and Health, Geneva, World Health Organization; 2001.